Who invented field hospitals?

The genesis of the field hospital—a temporary medical facility established close to the fighting—is not attributable to a single person or a singular moment of invention. Rather, it represents a gradual, often painful evolution in military logistics and humanitarian response spanning centuries, marked by periods of radical innovation interspersed with devastating setbacks. [1][6] Before organized systems took hold, battlefield care was rudimentary, relying heavily on individual surgeons’ abilities to improvise amidst chaos, often resulting in incredibly high mortality rates for the wounded who survived the initial injury. [9] The very term "field hospital" implies a system designed for mobility and proximity to action, a logistical feat that ancient armies struggled to maintain consistently. [1]
# Early Concepts
The need for medical support near combat zones is as old as organized warfare itself. Early attempts often involved simple aid stations or using structures like temples or barns near a battle site once fighting subsided. [6] Roman armies, for instance, had medical personnel, medici, who would treat soldiers, though their organization was not the same as the later, tiered system we recognize today. [1] The true precursor to the modern field hospital was the development of a system that categorized care based on the wound's severity and the soldier's immediate need for evacuation or stabilization. [8] This required not just doctors, but dedicated transport and administrative support, elements often missing in earlier eras. [6]
The development of fixed hospitals was easier to conceptualize and fund than truly mobile ones designed to follow armies across shifting terrain. Early military hospitals were frequently established in captured towns or large, static structures far removed from the front lines, meaning the journey itself was often the fatal factor for the severely wounded. [6] The concept needed a champion who could impose a standardized, scalable structure onto the messiness of active combat medicine.
# Civil War Structure
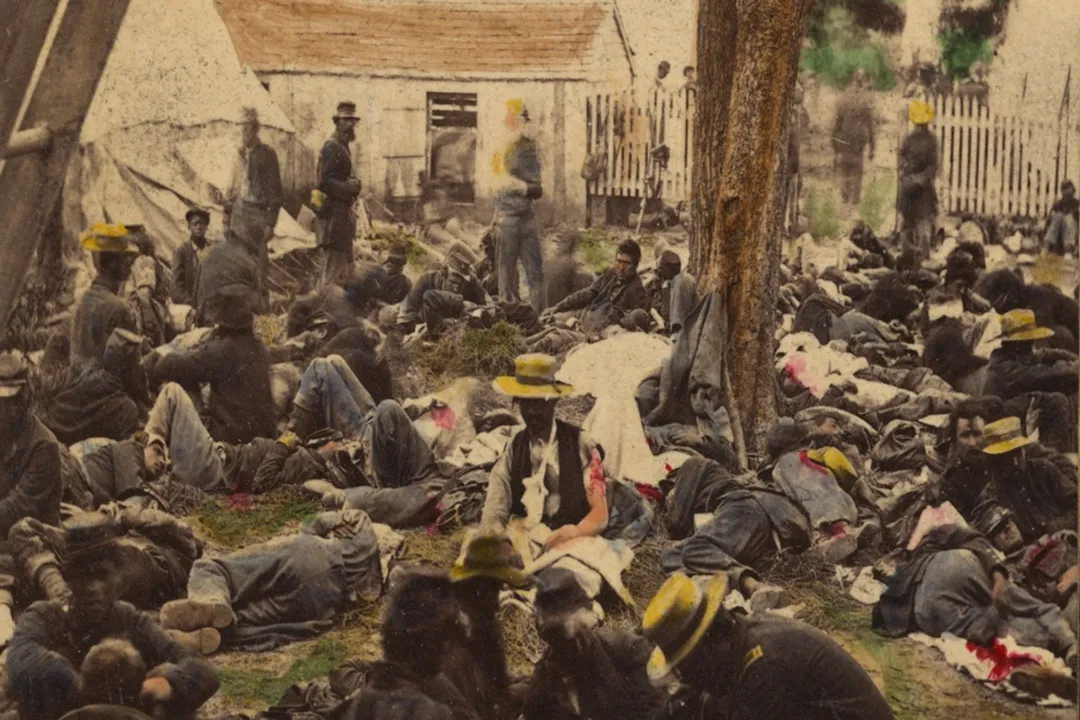
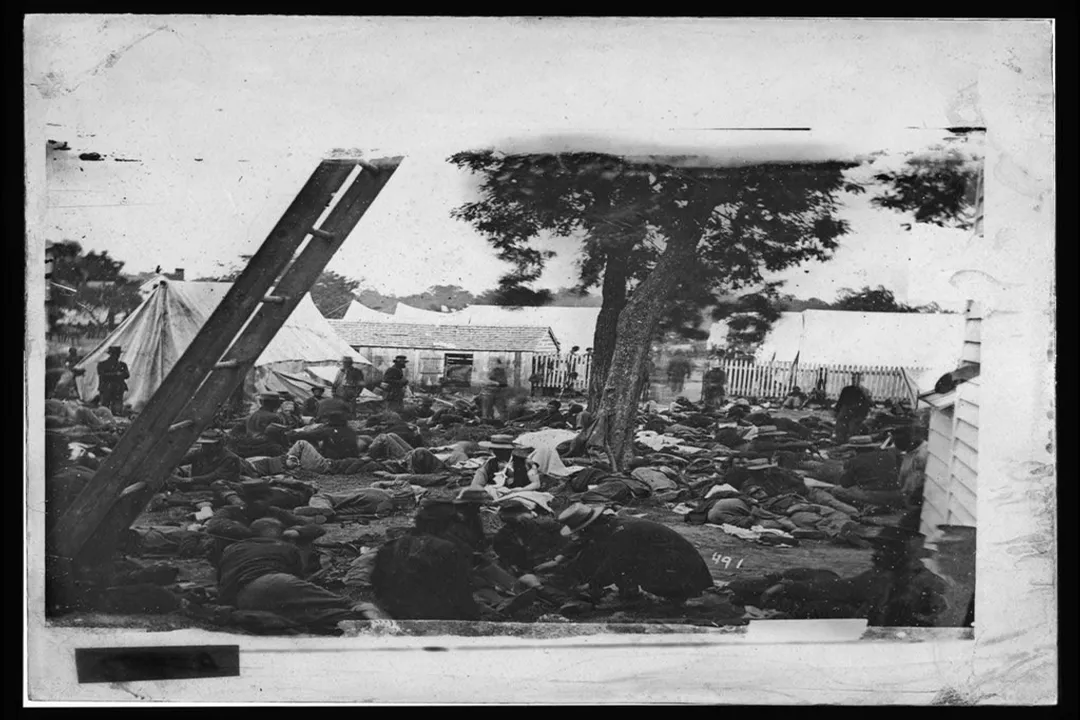
The American Civil War, fought in the mid-19th century, stands as a watershed moment in the history of battlefield medicine and the formalization of the field hospital structure. [2][9] The sheer scale of casualties during this conflict—with battles involving tens of thousands of men—overwhelmed all existing medical infrastructure, exposing critical deficiencies in organization. [9] Before systematic changes were implemented, the scene following a major engagement was grim: wounded soldiers lay where they fell for extended periods, and the transportation available was often inadequate, leading to preventable deaths from shock, exposure, or blood loss before any surgical intervention could occur. [2]
The sheer volume of amputations required, coupled with the poor sanitation inherent in temporary setups, made the early Civil War experience a disaster from a medical logistics standpoint. [9] While various medical staff worked tirelessly, the lack of a coordinated evacuation plan meant that surgical tents or rudimentary hospitals were often overwhelmed or improperly positioned relative to the fighting. [2]

# Letterman's System
If one figure must be associated with the invention of the functional, modern field hospital system, it is Major Jonathan Letterman, who served as the Medical Director of the Army of the Potomac starting in 1862. [5][6] Letterman did not invent the idea of a tent hospital, but he revolutionized the organization around it, effectively creating the logistical chain that defined future military medical care. [5] His contribution was less about a new surgical technique and more about administrative genius and supply chain management. [5]
Letterman introduced a clear, three-tiered system of care, which provided structure where previously there had only been ad hoc improvisation. [5][8] This standardization meant that every unit, regardless of where it was fighting, operated under the same operational rules for handling casualties.
The tiers of care he established were:
- Regimental Aid Stations: These were the first points of contact, often just a small group of surgeons and assistants near the line of battle, tasked with immediate resuscitation and control of bleeding—the absolute minimum required to keep a soldier alive long enough to move. [5]
- Division Field Hospitals: Located a safe distance behind the fighting, these were the actual field hospitals. They were stocked with supplies, staffed with more surgeons, and were responsible for more definitive care, including the many amputations necessitated by contemporary battlefield trauma. [2][5] Letterman ensured these hospitals were supplied via an organized wagon train system, ending the previous reliance on surgeons scrambling for local resources. [5]
- General Hospitals: These were fixed facilities, often located miles away in cities or established towns, serving as the final destination for those requiring long-term recovery or extremely complex procedures. [5]
This structured evacuation chain, which prioritized moving the wounded away from the immediate battlefield to specialized centers, is the bedrock upon which modern military medical organization rests. [1][8] Letterman's implementation involved creating standardized ambulance corps, meaning that organized transport was consistently available to ferry the wounded from the aid station to the field hospital, a critical departure from relying on private wagons or commandeered civilian transport. [5] This logistical focus—getting the right patient to the right level of care, quickly—is what truly defined the success of his system. [8]
# Formalizing Triage
A necessary component of any functional field hospital system is triage, the process of sorting casualties based on the urgency of their need for care versus their likelihood of survival. [3] While the concept of prioritizing patients existed before the Civil War, the scale of the fighting, combined with Letterman's organizational structure, forced its formal adoption and refinement. [3]
In the field hospital setting, triage meant making immediate, harsh decisions about resource allocation. A soldier with a minor, non-life-threatening wound might wait while one with a severe chest wound that had a slim chance of survival received immediate attention. [3] In the context of the Civil War field hospital, triage often devolved into sorting based on survivability after intervention: those who could likely be saved quickly were treated first, while those with wounds deemed fatal (like massive abdominal injuries without advanced surgical capability) might be provided palliative care or simply left until resources were available. [3][9]
It is worth noting a key distinction in early triage philosophy: contemporary battlefield EMS, as seen in modern contexts, often prioritizes saving the greatest number of lives with immediate, minimal intervention, sometimes allowing stabilization before transport. [4] Civil War field hospitals, due to the immense surgical loads, often favored rapid, definitive—though often brutal—intervention like amputation, as a way to clear beds and make immediate disposition decisions. [9]
If we analyze the shift, Letterman’s system wasn't just about where to treat, but how to manage the flow. Prior to this, the aid station was often the only surgical location, meaning surgeons operated under direct fire or extreme duress. [2] By establishing the division field hospital a sensible distance away, surgeons could work in a more stable environment, allowing for better preparation, sanitation (relative to the circumstances), and the application of standardized protocols, including triage. [5][8] This separation of the treatment area from the fighting area is a defining characteristic that distinguishes a true field hospital system from a mere collection of roadside surgeons.
# Global Adoption and Refinement
The success of the organized system pioneered during the American Civil War was not lost on subsequent military planners worldwide. [1][6] The lessons learned—especially regarding supply lines, standardized evacuation, and the need for tiered care—were studied by medical leaders in Europe and elsewhere. [6]
In the lead-up to and during the First World War, the development of field hospitals continued, adapting to new forms of trauma like machine gun fire and shell blasts. [7] The experience of WWI demonstrated the need for more tiers of care and greater specialization than the Civil War model required, as injuries became more complex (e.g., blast injuries, nerve damage) and the front lines were often more static for longer periods. [7] The field hospital evolved into larger, more specialized units: Casualty Clearing Stations (CCS) often took on the major surgical roles previously reserved for the division field hospitals, while smaller Advance Dressing Stations served the function of the original regimental aid stations. [1][7] This reflects a continuous trend: as warfare becomes more destructive, the medical system must become more layered and specialized to manage the resulting complexity of injuries. [8]
What the initial Civil War system provided was the template for movement and organization—a logistical apparatus designed to get mass casualties out of the kinetic zone—a concept that remained relevant even as the medical technology within those tents changed dramatically. [1][6] The sheer volume of medical material that needed to be tracked, from bandages to ether, necessitated the administrative clarity Letterman imposed, which is something even the most skilled historical battlefield doctors lacked the bureaucratic tools to manage effectively before the 1860s. [5]
# Logistics Over Medicine
One insight that becomes clear when studying the transition from rudimentary care to a formal system is that the invention of the field hospital as an effective institution was predominantly a logistical victory, not a medical one. [8] The core medical challenges—infection, hemorrhage, shock—remained largely constant for decades; what changed was the certainty of access to care within the "golden hour" or just beyond it. [4] An ancient surgeon might have possessed adequate knowledge for a wound on the spot, but without clean water, sterilized instruments (a concept not fully grasped), and reliable transport to a prepared site, that knowledge was frequently useless against overwhelming numbers. [9] Letterman’s genius lay in recognizing that the greatest threat to the wounded soldier was the system designed to help him, and he replaced that system with an efficient, accountable machine. [5] The physical tent or building was secondary; the efficient flow of the soldier from point of injury to surgical intervention was paramount. [1][4]

# The Implied Need for Distance
Another subtle element that shaped the evolution of the field hospital is the implicit recognition of the need for psychological and physical separation from the immediate danger. While the Civil War system sought to place the division hospital close enough for rapid transport, it had to be far enough away to avoid being overrun or bombarded. [2] Think of the difference in operational tempo: a surgeon at an aid station is constantly listening for the next incoming volley, making it impossible to focus on complex internal operations. The field hospital needed a degree of calm, even if temporary, to allow for procedures like amputation, which require time and a steady hand. [3] This necessary separation—the strategic placement of the medical infrastructure relative to the fighting—is a critical, non-medical decision that defines the utility of the field hospital concept. [1][6] If a facility is too close, it becomes a casualty itself; too far, and it becomes merely a destination hospital, defeating the purpose of "field" care.
# Modern Legacy
The concepts formalized in the mid-19th century continue to underpin global medical response today. Modern military medicine often uses Mobile Army Surgical Hospitals (MASH) or similar expeditionary units, which function on principles very similar to those established over a century ago: rapid deployment, high-volume throughput, and clear evacuation pathways. [1][8] Even civilian disaster response often mimics this tiered structure when overwhelmed resources require establishing temporary centers near incident sites. [4] The foundation remains the same: a temporary, organized structure designed to stabilize and process casualties quickly before they can overwhelm fixed facilities or succumb to delays. The "inventor" is therefore not a single person, but a succession of military planners who recognized that winning wars required managing the human cost with methodical, organized attention. [6]
In the end, the story of the field hospital is less about who first pitched a tent on a battlefield and more about who first figured out how to run the plumbing. It was the standardization of supplies, the establishment of defined roles for personnel at each level, and the creation of a dedicated, non-combatant transport corps that marked the real breakthrough. [5] This organizational achievement, primarily codified during the American Civil War, remains the enduring legacy of the modern field hospital system. [1][8]
Related Questions
#Citations
Field hospital - Wikipedia
Civil War-Era Hospitals | Behind the Lens: A History in Pictures - PBS
The Development of Triage - National Museum of Civil War Medicine
From Battlefield Medicine to Civilian EMS - National EMS Museum
Major Jonathan Letterman revolutionized military medicine during ...
History of Military Field Hospitals (Chapter 1)
Evolution of the Military Hospital - AMEDD Center of History & Heritage
Bernard John Dowling Irwin and the Development of the Field ...