Who invented clinical data warehouses?
Pinpointing the exact person who invented the Clinical Data Warehouse (CDW) is a deceptively complex question, much like asking who invented the modern skyscraper. Instead of a single lightbulb moment, the CDW arose from a convergence of technological advancements in data storage and the increasingly urgent, unique demands of patient care and medical research. Its lineage traces directly back to the broader concept of the data warehouse, a term established in the late 1980s and early 1990s.
# DW Origins
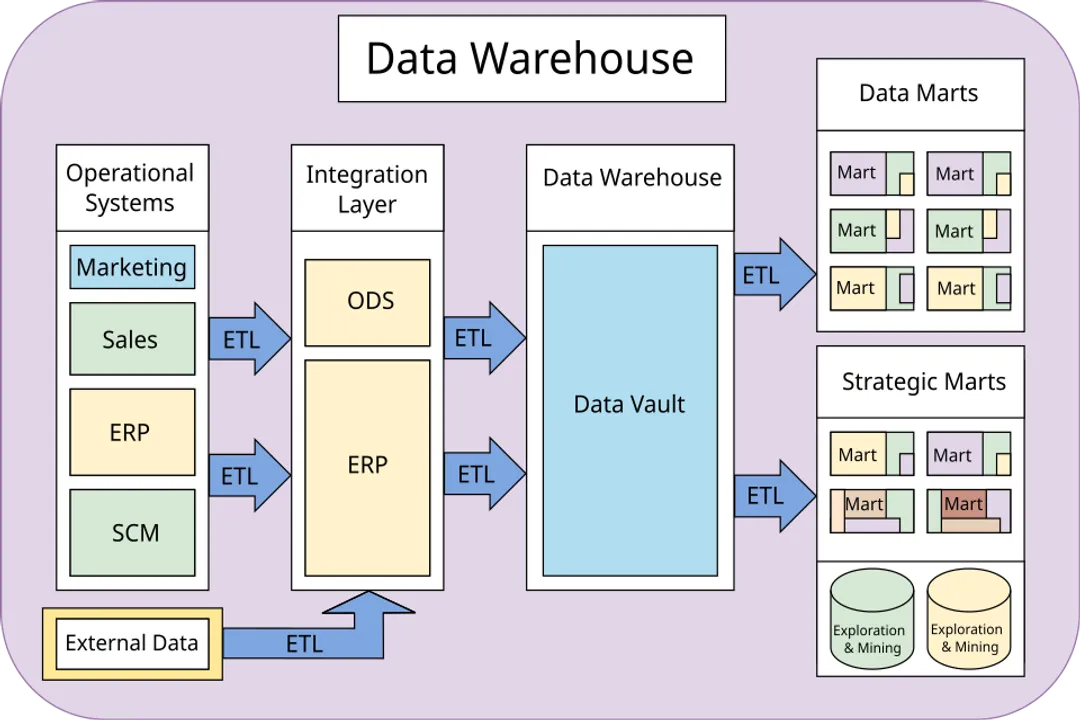
Before we could tackle clinical complexity, the foundational ideas of organizing vast, disparate data sets for analytical purposes had to be established. The conceptual father of the data warehouse is widely considered to be Bill Inmon, who defined it as a subject-oriented, integrated, time-variant, and non-volatile collection of data in support of management's decision-making process. This architectural blueprint—moving data out of transactional systems into a structure optimized for reporting—was the prerequisite for everything that followed in healthcare IT.
Following Inmon’s initial vision, other methodologies emerged, notably the bottom-up approach championed by Ralph Kimball, which favored the use of dimensional modeling built around data marts. These two schools of thought shaped the architectural debates for the next decade across all industries, including healthcare. The core idea, regardless of methodology, was to transform raw operational data into information usable for strategic insight.
The general data warehouse (DW) provided the technological possibility. However, healthcare data presented an entirely different set of challenges that necessitated a specialized structure, which we now call the CDW.
# Clinical Demands
The transition from a generic DW to a Clinical Data Warehouse required overcoming hurdles specific to medical environments. Traditional business data deals in defined metrics like sales volume or inventory levels. Clinical data, conversely, is characterized by high volume, extreme heterogeneity, and inherent messiness. Think about unstructured physician notes, varying coding standards across departments, and time-series data reflecting physiological changes minute-by-minute.
One major driver for CDW development was the need to aggregate information that was traditionally siloed. Patient data often resided in separate systems for the Emergency Department, Inpatient Services, Radiology, and Pharmacy, making a single, longitudinal view of a patient impossible for quality improvement or research. To truly understand patient outcomes, researchers and administrators needed an integrated, historical record.
This need wasn't just about quantity; it was about quality and context. For instance, a general DW might track the sale of a drug. A CDW must track who got the drug, why (the diagnosis), when (timing relative to the illness progression), and what happened next (the outcome or adverse event). This deep contextual linkage is what separates a simple database dump from a functional clinical warehouse.
# Repository Differentiation
In trying to manage these complex needs, the term Clinical Data Repository (CDR) often surfaces alongside CDW, sometimes causing confusion regarding who "invented" what. While both deal with clinical data, their primary functions differ, which reveals a bit about the chronological development of data management in hospitals.
A CDR is often defined as a structure designed for the near-real-time collection of clinical data, primarily serving operational needs like providing clinicians with up-to-date patient information at the bedside. Its focus is operational support and data integration from source systems.
In contrast, the CDW is built specifically for analysis and reporting over long periods. It takes the integrated data from the CDR (or directly from source systems) and restructures it—often using dimensional models—to answer questions about populations, trends, and effectiveness of care across months or years. If the CDR is the real-time nervous system, the CDW is the long-term memory designed for learning. The historical necessity was first to manage the raw flow (the repository function), and then to analyze the flow retrospectively (the warehouse function).
# The Dawn of Clinical Warehousing
The initial realization that a specialized analytical structure was necessary seems to have emerged in the mid-to-late 1990s, coinciding with the broader acceptance of the DW concept and the increasing volume of Electronic Health Record (EHR) data available for extraction. The "invention" of the CDW, therefore, belongs not to a single individual, but to the early pioneering IT departments and healthcare systems that began applying Inmon’s and Kimball’s principles directly to clinical records.
Early attempts often involved building custom data marts for specific departments, like cardiology or finance, but the recognized value came when systems began integrating these silos. Source material suggests that by the early 2000s, health systems were actively sharing "lessons from 20 years" of experience, confirming that the structured approach to clinical analytics was already maturing.
Consider the difference in data structure required for a simple hospital administrative task versus a public health study. Administrative reporting might require summary tables of procedures performed last month—something a well-structured operational data store could handle. A public health study, however, might need to track the long-term survival rates of patients receiving a specific treatment across five different hospital sites over a decade, adjusting for comorbidities documented years apart. This level of longitudinal, integrated querying is the clinical data warehouse requirement, and its widespread adoption marks the beginning of the CDW as a distinct entity.
A key element in these early successes was defining the data model appropriately. One significant paper discussing data warehousing in healthcare emphasized the importance of a flexible, iterative approach to modeling, acknowledging that clinical domain knowledge must guide the technical structure—a lesson learned through early failures where purely technical models did not serve clinical questions.
| Characteristic | General Data Warehouse (DW) | Clinical Data Warehouse (CDW) |
|---|---|---|
| Primary Goal | Supporting business decision-making | Supporting clinical quality, research, and population health |
| Data Nature | Structured transactional data | High volume, heterogeneous, time-series data (e.g., unstructured notes, vitals) |
| Time Horizon | Short to medium-term trends | Long-term longitudinal patient history |
| Key Challenge | Data integration and transformation | Semantic complexity and data context retention |
This comparison highlights that the "invention" was not the technology itself, but the contextual application of that technology to uniquely difficult medical information. It required the expertise of both data architects and clinical domain specialists working together.

# Governance and Scope Expansion
The evolution of the CDW also brought governance issues to the forefront, a natural consequence of centralizing sensitive patient information. As these warehouses became more central to quality reporting and research, the need for strict controls over data access and interpretation became paramount. A clinical data warehouse must adhere to privacy regulations, meaning the implementation is inherently tied to ethical and legal compliance, a factor largely absent from initial, general DW projects.
Projects involving CDWs often require navigating complex institutional politics. For example, a hospital system might start with a CDW focused on reducing readmission rates for a specific disease cohort, building out the necessary data models for labs, medications, and discharge summaries. If this initial project is successful, the scope naturally expands to include data from affiliated clinics or different specialty areas, demanding increasingly sophisticated governance to ensure data standards remain consistent across all new feeds. This phased, goal-oriented expansion, rather than a single massive deployment, characterized the practical emergence of the CDW in many large organizations.
It is insightful to consider that the true "inventor" of the successful CDW was perhaps the governance board that demanded verifiable, accurate data for accreditation or public reporting. Without this external pressure from regulatory bodies or institutional quality goals, the investment to clean and integrate complex clinical records might never have been made, leaving healthcare stuck with isolated, operational data marts.
# Lessons from Longevity
Looking back over two decades of health data warehousing experience reveals a crucial insight about invention versus maturation. The initial architecture, focused on creating a single source of truth, has proven durable, yet the specific technologies and analytical layers built upon it are in constant flux.
Early CDWs might have struggled significantly with data latency—the delay between an event happening (a lab result being finalized) and it appearing in the warehouse for analysis. Modern demands, especially for real-time clinical decision support, push the concept closer to streaming analytics, but the core warehousing function remains essential for retrospective analysis. Systems that succeeded learned to manage this trade-off: prioritizing the high-integrity, historical structure of the warehouse while building out separate, faster operational layers where necessary.
Another key lesson learned through this evolution pertains to the data source itself. The shift from coded, structured data entry (like ICD-10 codes) to richer documentation within EHRs forced CDW architects to incorporate techniques for handling unstructured data, such as Natural Language Processing (NLP) to extract concepts from clinical notes. An early CDW designed before NLP maturity would have missed a huge percentage of vital clinical context contained in narrative text. This adaptability, incorporating emerging data science techniques into the established warehouse structure, is the hallmark of a mature CDW environment.
From a practical standpoint, anyone looking to build or refine a CDW today should remember that the foundational architecture (the Inmon/Kimball legacy applied clinically) is established, but the value realization depends entirely on the quality of the extraction and transformation logic applied to specific, messy clinical workflows. A useful tip for current practitioners is to always model the time dimension of clinical events with extreme precision—not just the date a record was entered, but the actual time the event occurred (e.g., time of drug administration, time of blood draw). This level of granularity is often overlooked in initial builds but becomes the source of endless frustration years later when trying to correlate interventions with rapidly evolving patient states.
In summary, the invention of the Clinical Data Warehouse was not a singular event credited to one person. It was an evolutionary necessity driven by the unique complexity of biomedical data, architecturally enabled by the foundational work of data warehousing pioneers like Inmon and Kimball, and ultimately realized by healthcare systems willing to integrate operational data with analytical rigor to improve patient outcomes and advance medical understanding.
Related Questions
#Citations
Data warehouse - Wikipedia
Development of a clinical data warehouse from an intensive care ...
The Healthcare Data Warehouse: Lessons from the First 20 Years
Wang | Clinical Data Warehousing: A Scoping Review
Development of a clinical data warehouse from an intensive care ...
Clinical Use of an Enterprise Data Warehouse - PubMed Central - NIH
Implementation of data access and use procedures in clinical data ...
The development and use of data warehousing in clinical settings
Clinical Data Warehouse